Our Services

Services
Antrostomy
It is also often done in combination with a Functional Endoscopic Sinus Operations.
It is a relatively minor procedure and the patient is usually discharged the same day with great relief if the sinuses were filled with fluids.
This is temporary in nature and should be substituted by a more formal sinus operation if indicated.
Bone-Anchored Hearing Aid
USE AND OPERATION
Bone-anchored hearing aids use a surgically implanted abutment to transmit sound by direct conduction through bone to the inner ear, bypassing the external auditory canal and middle ear. Titanium prosthesis is surgically embedded into the skull, approximately 3cm to the back of the earlobe, at the top limit of the lobe, with a small abutment exposed outside the skin. A sound processor sits on this abutment and transmits sound vibrations to the titanium implant. The implant vibrates the skull and inner ear, which stimulate the nerve fibres of the inner ear, allowing hearing.
The implant is done via a small procedure that requires only day clinic facility. The screw is left for three months to seat whereafter the hearing aid is attached to the screw. The size of the hearing aid is approximately 2cm x 1cm square.
It relays the sound through bone and therefore leaves the ear canal open. Quite often with conventional hearing aids the ear canal tends to suppurate. It also enables people who have a one-sided hearing loss to have the BAHA placed on the dead ear’s side. The sound is then received on that side and in real-time relayed through the scull to the other ear, which enables the person to have near normal hearing as far as stereo and sound localization abilities are concerned.
This is not a substitute for a conventional hearing aid, but rather an adjunct in certain instances.
BENEFITS
The benefits of Bone Anchored Hearing Aid such as BAHA are well documented. By bypassing the outer or middle ear, BAHA can increase hearing in noisy situations and help localise sounds. The benefit is not only improved speech understanding, hearing with BAHA results in a natural sound with less distortion and feedback when compared with conventional hearing aids. The ear canal is left open for comfort, and helps to reduce any problems caused by chronic ear infections or allergies. In patients with Single-sided sensorineural deafness (SSD), BAHA sends the sound via the skull bone from the deaf side to the inner ear of the hearing side. This transfer of sound gives a 360-degree sound awareness.
For further information the practice can be contacted.
Bronchoscopy
PURPOSES
Diagnostic:
To view abnormalities of the airway
To obtain tissue specimens of the lung in a variety of disorders. Specimens may be taken from inside the lungs by biopsy, bronchoalveolar lavage, or endobronchial brushing.
To evaluate a person who has bleeding in the lungs, possible lung cancer, a chronic cough, and sarcoidosis.
Therapeutic:
To remove secretions, blood, or foreign objects lodged in the airway
Laser resection of tumours 9or benign tracheal and bronchial strictures
Stent insertion to palliate extrinsic compression of the tracheobronchial lumen from either malignant or benign disease processes
Bronchoscopy is also employed in percutaneous tracheostomy
Tracheal intubation of patients with difficult airways is often performed using a flexible bronchoscope.
PROCEDURE
A flexible bronchoscope is inserted with the patient in a sitting or supine position. Once the bronchoscope is inserted into the upper airway, the vocal cords are inspected. The instrument is advanced to the trachea and further down into the bronchial system and each area is inspected as the bronchoscope passes. If an abnormality is discovered, it may be sampled, using a brush, a needle, or forceps. Specimen of lung tissue (trans bronchial biopsy) may be sampled using a real-t8ime x-ray (fluoroscopy). Flexible bronchoscopy can also be performed on intubated patients, such as patients in intensive care. In this case, the instrument is inserted through an adapter connected to the tracheal tube.
Dacryocystorrhinostomy
TREATMENT
Traditional:
A small incision is made on the side of the nose and some bone is removed to make a connection to the nose. Drains are then placed from the eye into the nasal cavity to facilitate the drainage. However in recent years we are using a trans nasal endoscopic operation with no incisions on the outside. It is sometimes done in conjunction with an Ophthalmic Surgeon, although Ear, Nose and Throat Surgeons that do a lot of these operations do the eye part as well. A small polythene tube is placed through the nose into the medial part of the eye and back through the other lacrimal opening into the nose. This is left in place for approximately three to six months.
It has no side effects on the patient.
This is a technically difficult operation and should only be done by people with experience in this field for maximum chance of good results.
Direct Laryngoscopy
When a Direct Laryngoscopy is done, an instrument is done an instrument is placed through the mouth with the head extended. A microscope is then used to look through the instrument at the various sites.
Vocal cords etc., can be visualised very adequately. It leaves the operator with two free hands. Micro-instruments, on extended stilts, are used to either physically remove or take biopsies.
The laser is often connected to the microscope and used through the scope to vaporise or operate the vocal cords and other areas in the pharynx.
An Ear, Nose and Throat anaesthetist is necessary to manage the shared airway that is used.
Postoperatively, depending on what type of surgery was done, a bit of discomfort in the throat is experienced. Sometimes, if a biopsy has been taken from the vocal cords, some hoarseness can be experienced until the cord has healed. Usually this operation does not need an overnight stay and the patient can go back to work within a day or two.
It is essential for any potentially malignant pathology to have this procedure done so that visualization can be achieved and biopsies can be taken.
Exostosis Removal
Transcanal removal with an osteotome involves no incisions behind the ear; the surgery is done entirely through the ear canal. This seems desirable to some patients, since it suggests a faster healing time, which means they’ll be able to get back into the water and surf sooner. Exostoses are often removed with a high speed ear drill. They are drilled down to their normal height with good visualization and in specialist’s hands; this operation carries a low risk of damage to the ear or the related nerves and a good result.
Obviously if continuous exposure to cold water etc, they may reform, although this is a long term process.
Foreign bodies in the ear, nose and airway
FOREIGN BODIES IN THE EAR;
Foreign bodies can either be in the ear lobe or in the ear canal. Objects usually found in the ear lobe are earrings, either stuck in the lobe from infection or placed too deep during insertion. Foreign bodies in the ear canal can be anything a child can push into his/her ear. Some of the items that are commonly found in the ear canal include the following:
Food
Insects
Toys
Buttons
Pieces of crayon
Small batteries
It is important for parents to be aware that children may cause themselves or other children great harm by placing objects in the ear.
WHAT ARE THE SYMPTOMS OF FOREIGN BODIES IN THE EAR?
Some objects placed in the ear may not cause symptoms, while other objects, such as food and insects, may cause pain in the ear, redness, or drainage. Hearing may be affected if the object is blocking the ear canal.
TREATMENT FOR FOREIGN BODIES IN THE EAR;
The treatment for foreign bodies in the ear is prompt removal of the object by your child’s physician. The following are some of the techniques that may be used by your child’s physician to remove the object from the ear canal;
Instruments may be inserted in the ear,
Cleaning the ear canal with water,
A machine with suction to help pull the object out.
After removal of the object, your child’s physician will then re-examine the ear to determine if there has been any injury to the ear canal. Antibiotic drops for the ear may be prescribed to treat any possible infections.
FOREIGN BODIES IN THE NOSE
Objects that are put into the child’s nose are usually soft things. These would include, but are not limited to, tissue, clay, and pieces of toys or erasers. Sometimes, a foreign body may enter the nose while the child is trying to smell the object. Children often place objects in their noses because they are bored, curious, or copying other children.
WHAT ARE THE SYMPTOMS OF FOREIGN BODIES IN THE NOSE?
The most common symptom of a foreign body in the nose is nasal drainage. The drainage appears only on the side of the nose with the object and often has a bad odour. In some cases, the child may also have a bloody nose.
TREATMENT FOR FOREIGN BODIES IN THE NOSE;
Treatment of a foreign body in the nose involves prompt removal of the object by your child’s physician. Sedating the child is sometimes necessary in order to remove the object successfully. This may have to be performed in the hospital, depending on the extent of the problem and the cooperation of the child.
The following are some of the techniques that may be used by your child’s physician to remove the object from the nose:
Suction machines with tubes attached, instruments may be inserted in the nose. After removal of the object, your child’s physician may prescribe nose drops or antibiotic ointments to treat any possible infections.
FOREIGN BODIES IN THE AIRWAY
A foreign body in the airway (choking) constitutes a medical emergency and requires immediate attention. The foreign body can get stuck in many different places within the airway. According to the American Academy of Paediatrics, death by choking in children occurs most often in children younger than 5 years. Infants younger than 1 year old account for two-thirds of child choking victims.
Children between the ages of 7 months and 4 years are in the greatest danger of choking on small objects, including, but not limited to, the following:
Seeds
Toy parts
Grapes
Hot dogs
Pebbles
Nuts
Buttons
WHAT ARE THE SYMPTOMS OF FOREIGN BODIES IN THE AIRWAY?
Foreign body ingestion requires immediate medical attention. The following are the most common symptoms that may indicate a child is choking. However, each child may experience symptoms differently. Symptoms may include:
Choking or gagging when the object is first inhaled,
Cough at first,Wheezing (a whistle sound, usually made when the child breathes out).
Although the initial symptoms listed above may subside, the foreign body may still be obstructing the airway. The following symptoms may indicate that the foreign body is still causing an airway obstruction:
Stridor (a high pitched sound usually heard when the child breathes)
Cough that gets worse
Child is unable to speak
Pain in the throat area or chest
Hoarse voice
Blueness around the lips
Not breathing
The child may become unconscious
TREATMENT FOR FOREIGN BODIES IN THE AIRWAY;
Treatment of the problem varies with the degree of airway blockage. If the object is completely blocking the airway, the child will be unable to breath or talk and his/her lips will become blue. This is a medical emergency and you should seek emergency medical care. Sometimes, surgery is necessary to remove the object. Children that are still talking and breathing but show other symptoms also need to be evaluated by a physician immediately.
Functional Endoscopic Sinus Surgery
Have you been troubled by sinus problems? Maybe you have frequent pain or pressure in your head or face. Maybe you have a hard time breathing through your nose. Or, perhaps you find you can no longer smell dinner cooking. If you have sinus trouble that doesn’t respond to medications, endoscopic surgery may offer relief. This procedure gives your doctor access to your sinuses through a tool called endoscope. Read on to learn more.
What Causes Sinus Problems?
Sinuses are hollow, air-filled chambers within the bones of your face and head. Problems develop when these chambers are blocked and can’t drain properly. Causes of blockage include colds or other infections, allergies, or obstructions in the nose.
Symptoms of Sinus Problems
Sinus problems can cause symptoms such as:
- A constantly runny nose
- Loss of sense of smell
- Nasal congestion
- Trouble tasting food
- Fullness in the ears
- Frequent headaches
- Green, yellow, or bloody drainage from the nose
- Facial pain
- Recurrent infections
- Trouble sleeping
How Sinus Surgery Can Help
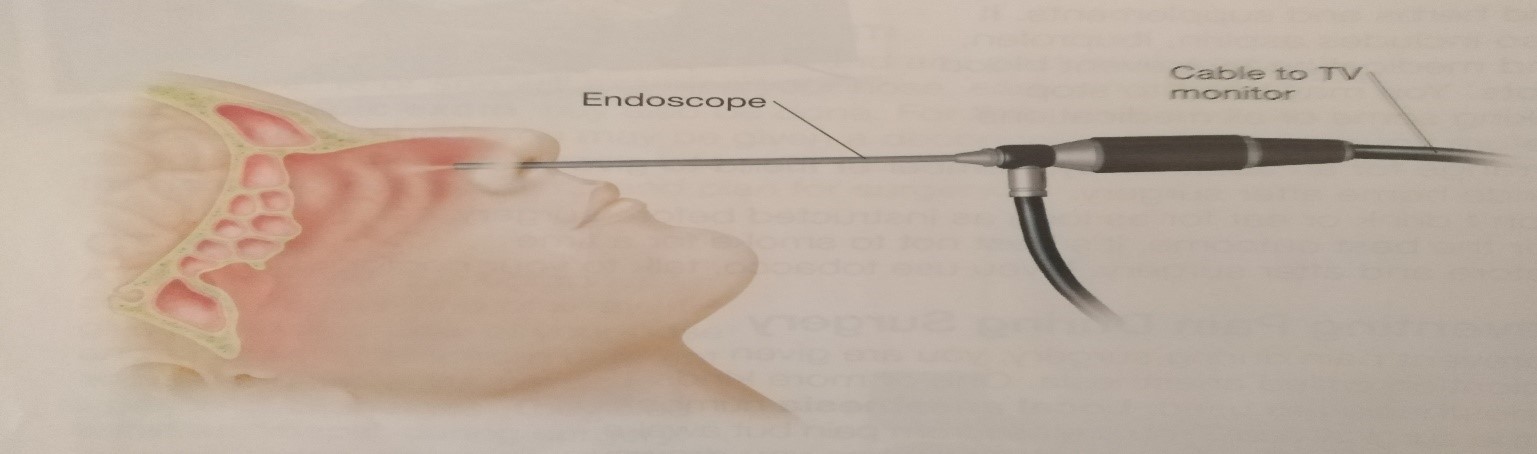
Endoscopic sinus surgery is preformed through the nose without any external incisions. A tool called an endoscope is used. This is a thin, flexible or rigid tube put through the nose into the sinuses. It gives the surgeon a clear, magnified view so he or she can find and treat nose and sinus problems.
Be Informed
Endoscopic surgery can treat your nose and sinus problems. But be sure you have all your questions answered before you decide on surgery. Know what the procedure can and cannot do for you. Discuss any nonsurgical options you haven’t tried. Be clear what the risks are for you. And know what you need to do to prepare for surgery and recover from it. By being informed, you can help your doctor ensure that your needs are met.
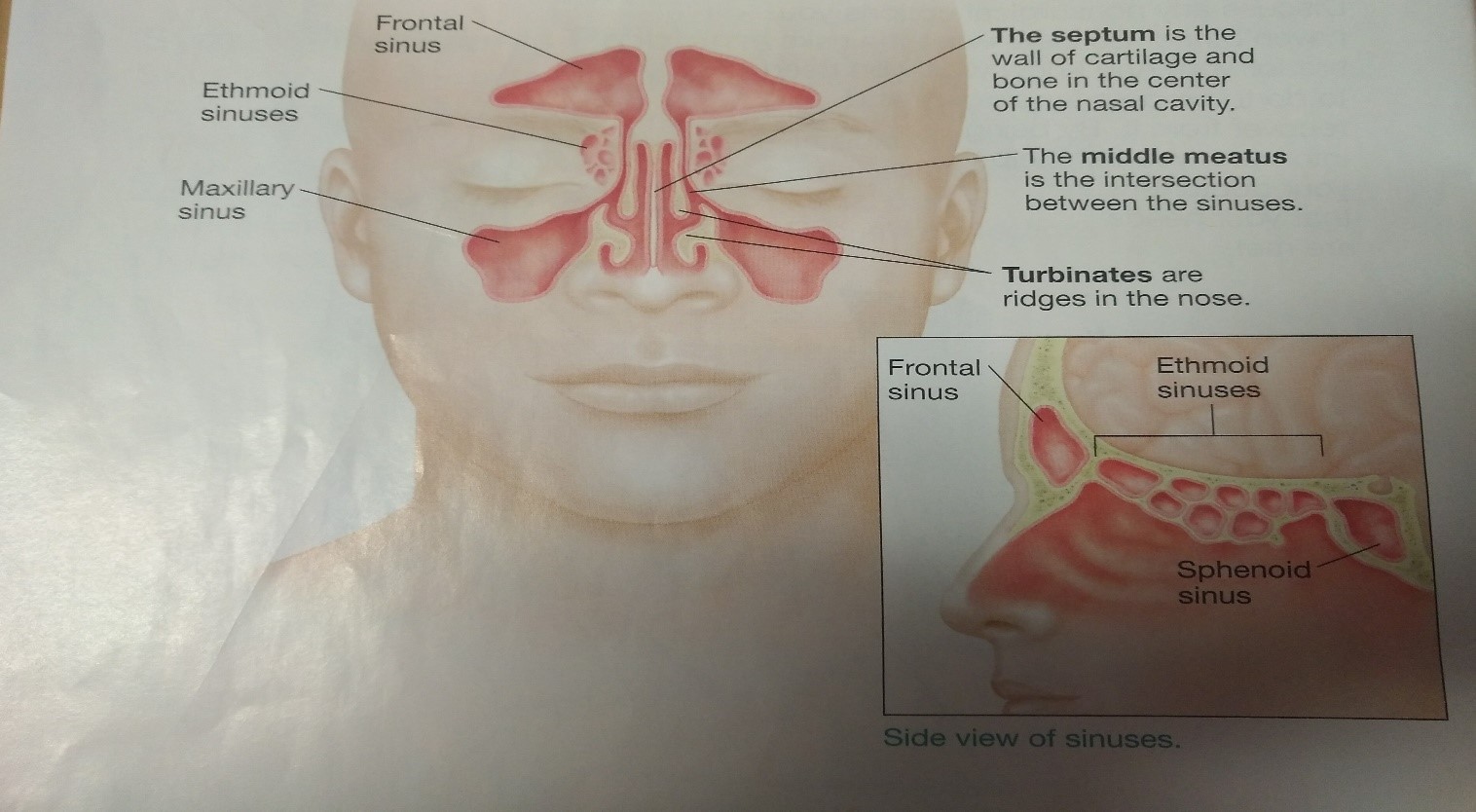
The Sinuses: A Drainage System
Sinuses are air-filled, hollow chambers within the bones of the face and head. The sinuses make a thin layer of a fluid called mucus. When sinuses are healthy, mucus drains freely into the nose. If this drainage path becomes blocked, infection can result.
Healthy Sinuses
Mucus moistens the nose and sinuses. It also helps to trap and remove dust, bacteria, and viruses from the nasal passages. The four pairs of sinuses drain mucus into the nasal cavity through small openings. In healthy sinuses, the drainage path is clear and open.
{kind=link}
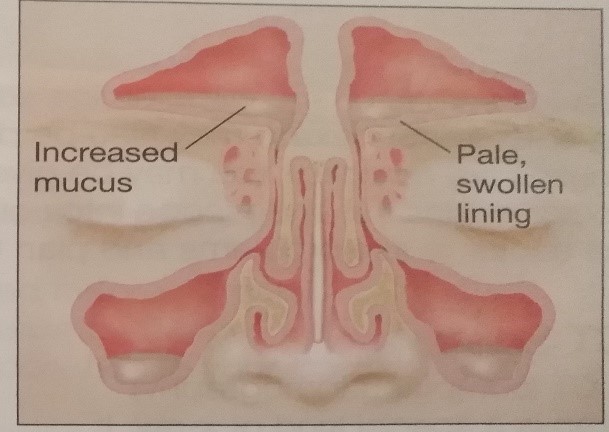
Blocked Sinuses
If drainage passages in the nose or sinuses are blocked, mucus cannot drain. Mucus-filled sinuses often become infected.
Colds and Other respiratory Infections cause the nose and sinus lining to make more and thicker mucus. The lining also swells. Mucus becomes trapped, which can lead to infection.
{kind=link}
Allergies irritate nasal and sinus tissues, such as turbinates. This causes swelling and blockage. Over time, irritation can cause polyps to form.
{kind=link}
Polyps develop when the lining of the nose or sinus swells and pushes out, forming a sac. Polyps likely form due to irritation. They can block drainage.
{kind=link}
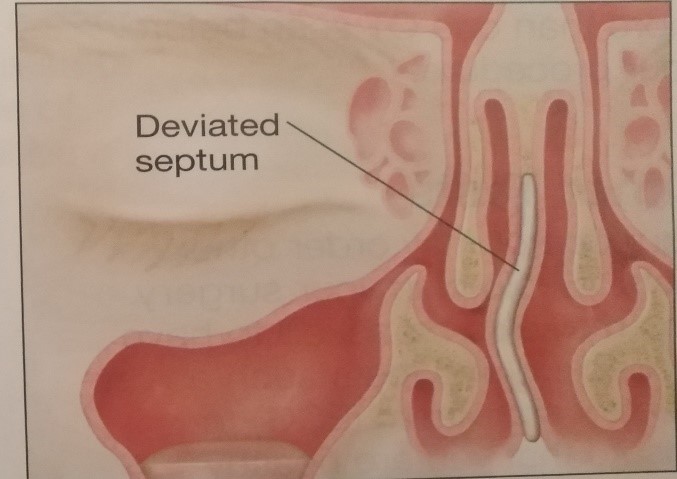
A deviated (crooked) septum may block nasal passages. The septum may have been injured. Or it may have formed with a bend in it.
{kind=link}
Before Surgery
Before surgery, your doctor may send you for a CT scan or other tests. Prepare for your surgery as instructed. If you have questions or concerns, call your doctor’s office.
History and Endoscopic Exam
Tell your doctor about your symptoms and any past treatments you’ve had. He or she will examine your nose, ears and throat. An endoscopic exam may also be done. For this, your nose and sinuses are numbed. You may be given a decongestant. Then the doctor guides the endoscope into your nasal passages. This allows the doctor to see problems and plan for surgery.
CT Scan
A CT (computed tomography) scan is a special kind of x-ray. It gives a detailed view of your nose and sinuses. Scan from different angles help show the precise location of blockages. They also serve as “maps” during surgery. In some cases, you may need more than one CT scan before your procedure.
Other Tests
Your doctor may order other tests to help plan your surgery. You may also be asked to have a check-up and tests such as an electrocardiogram (ECG) to ensure that you are healthy enough for surgery.
Front (coronal) view of a Deviated septum and blocked Sinus
{kind=link}
Preparing for Surgery
- Tell your doctor about ALL the medications you take. This includes over-the-counter drugs and herbs and supplements. It also includes aspirin, ibuprofen, and medication to prevent blood clots. You may need to stop taking some or all medications before surgery.
- Arrange for an adult family member or friend to give you a ride home after surgery.
- Don’t drink or eat for as long as instructed before surgery
- For the best outcome, its best not to smoke for a time before and after surgery. If you use tobacco, talk to your doctor.
Preventing Pain During Surgery
To prevent pain during surgery, you are given medication called anaesthesia. One or more kinds of anaesthesia are used. Local anaesthesia numbs just the surgical area. You are free from pain but awake and aware. Monitored sedation makes you drowsy or slightly asleep but doesn’t put you into a deep sleep. General anaesthesia puts you into a state like deep sleep for the procedure. The type of anaesthesia you will receive, and its risks will be discussed with you before surgery.
Risks and Complications
Endoscopic surgery is very safe. But it does have risks. These include:
- Infection
- Bruising
- Excessive bleeding
- Altered sense of smell or taste
- Damage to a tear duct
- Spinal fluid leakage (very rare)
- Vision loss (very rare)
During Surgery
Your surgeon views images from the endoscope during the surgery. Other instruments are used with the endoscope to perform treatment. Often, more than one area of the nose and sinuses is treated.
{kind=link}
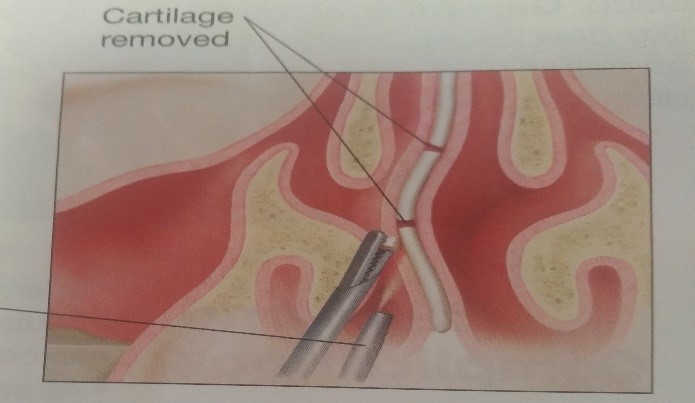
Straightening the Septum
To fix a deviated septum, your surgeon reshapes or trims the cartilage and bone that divides the nose. This creates more breathing space. Enough support remains for the nose to hold its shape. Cartilage may be removed to reshape and straighten the septum
{kind=link}
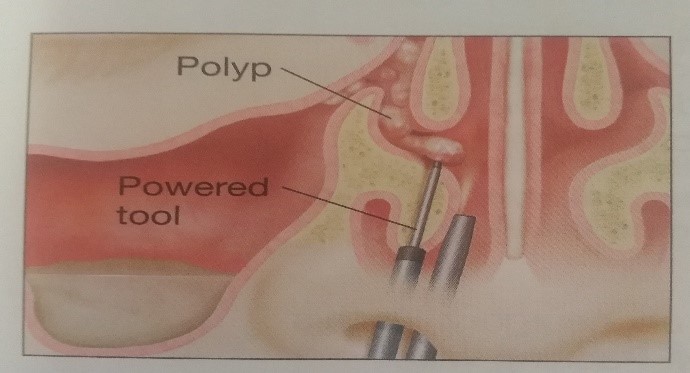
Removing Polyps
Polyp tissue can be removed in several ways. In many cases, the surgeon uses powered instruments. These helps remove polyps with minimal harm to nearby tissues. Polyps are removed using a powered Tool inserted next to the endoscope.
{kind=link}
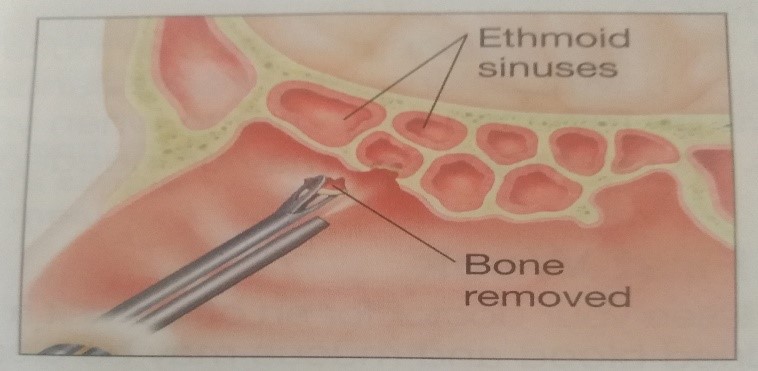
Opening the Ethmoid Sinuses
The ethmoid sinuses are made of many air sacs. These drains into the nasal cavity. If drainage is blocked, the surgeon may open the thin walls of bone that separate the air sacs to create a new path for mucus to drain. Pieces of bone are removed to open a path in the ethmoid sinuses.
{kind=link}
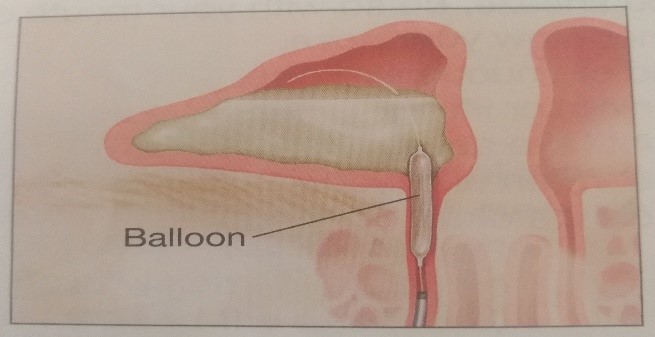
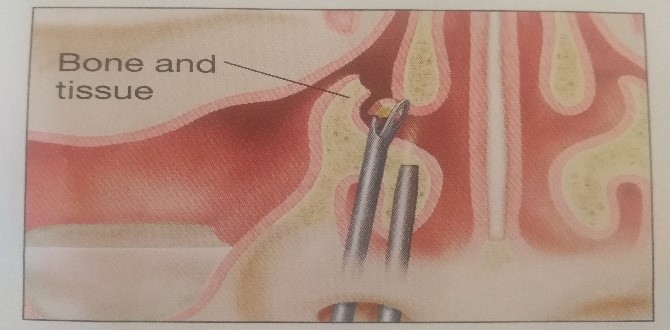
Clearing Nasal Passages
If drainage from the maxillary sinus is blocked, the surgeon may remove bone and tissue to clear a path. In some cases, a tiny balloon is inflated in the nasal passage (balloon sinuplasty). The goal is to widen the pathway and improve drainage.
Bone and tissue are removed to Improve drainage.
{kind=link}
Nasal passages are widened by inserting and inflating a small balloon.
{kind=link}
Your Recovery
You can often go home soon after surgery. Once you’re home, follow all your doctor’s instructions. Take an active role in your recovery to speed healing and prevent problems.
After Surgery
After surgery, you’ll be moved to recovery room. You may feel groggy from the anaesthesia and will likely have some discomfort. There will be a dressing under your nose to absorb drainage. You may also have packing (absorbent bandage) inside your nose. You will be released to go home when you’re stable. In certain cases, an overnight stay may be needed.
The First Week
You will see your doctor for an office visit a few days after surgery. At this visit, dried blood and mucus may be cleared away. If packing was used, which is not often, it will likely be removed. after this, care for your nose and sinuses as instructed. This includes:
- Rinse your nose and sinuses with saline as directed.
- Take medications as prescribed.
- Drink plenty of water.
To help prevent bleeding and promote healing:
- If you sneeze, do so with your mouth open.
- Do not blow your nose hard.
- Avoid strenuous exercise, straining, or lifting.
- Do not take Aspirin or Ibuprofen until you are told its okay.
Follow all instructions you are given for recovery, including taking your medications as directed.
As you heal, your stuffiness will decrease and you’ll breath more freely. Then you can enjoy life’s simple pleasures, like the smell of a home-cooked meal.
When to call your Doctor:
For about a week, some pinkish or dark red drainage is okay. But call your doctor if you have:
- A large amount of bright red bleeding,
- Drainage that is yellowish or greenish,
- Fever of (38ºC) or higher,
- Changes of vision,
- Swelling around the eye,
- A constant headache or increasing pain,
- Drainage of a large amount of clear fluid,
- Extreme tiredness or a stiff neck.
Dr Rossouw has done more than 6000 of these operations in the last 25 years. In 1988 he has spent some time in Graz in Austria with the founder of this technique, Prof. Messerklinger, as well as his protégé, Prof. Heinz Stamberger. He has since attended numerous courses across the globe in connection with this particular procedure.
Functional Endoscopic Sinus Surgery (FESS) is the mainstay in the surgical treatment of sinusitis and nasal polyps, including bacterial, fungal, recurrent acute and chronic sinus problems. Ample research supports its record of safety and success.
FESS is a relatively recent surgical procedure that uses nasal endoscopes (using Hopkins rod lens technology) through the nostrils to avoid cutting the skin. These endoscopes have diameters of 4mm (adult use) and 2.7mm (paediatric use) and come in varying angles of view from 0 degrees to 30, 45, 70, 90, and 120 degrees. They provide good illumination of the inside of the nasal cavity and sinuses.
FESS came into existence because of pioneering work of Messerklinger and Stamberger (Graz, Austria.) other surgeons have made additional contributions (first published in USA by Kennedy in 1985).
TECHNIQUE
There are four sinuses dealt with by means of this surgery: The frontal sinuses located in the forehead, the maxillary sinuses in the cheeks, the ethmoid sinuses between the eyes, and finally the sphenoid sinuses located in the back of the nasal cavity at the base of the skull.
MAXILLARY SINUS
One of the most accepted means of functionally enlarging the maxillary ostium is to perform an uncinectomy via the “swing door “technique. This initially removes the vertical process of the uncinate via backbiter inferiorly and sickle knife superiorly. The uncinate is swing medially and then severed at its lateral attachment. This is followed by a submucosal removal of the horizontal process of the uncinate and subsequent trimming of the mucosa to fully visualize the maxillary os.
Controversy exists as to whether or not the maxillary ostium should be enlarged or not depending on the disease status of the maxillary sinus. However, the medical literature would support a wide antrostomy and complete clearance down to healthy mucosa if fungal mucin is present within the sinus. In this circumstance, the ostium is enlarged superiorly to orbital floor and posteriorly to posterior fontanelle to allow wide access for clearance.
Complete maxillary debridement can be accomplished via either trans-ostial clearance which can be quite tedious. A new technique, canine fossa trephination, can accomplish this same task faster and with few side effects.
EXTENDED APPROACHES
More recently, the paranasal sinuses have been found to be a relatively low-morbidity approach to selected tumours of the anterior and posterior cranial fossa.
Endoscopic access to pituitary tumours has been found to be quite useful as well. Use of endoscopes for hypophysectomy allows excellent visualization within the sell and more complete tumor removal than would be available via microsurgical technique.
This can be divided into:
Approaches to the anterior cranial fossa
Approaches to the mid cranial fossa
Approaches to the posterior cranial fossa
Access to the infratemporal fossa (incl. pterygopalatine fissure)
Access to the sella turcica
Orbital access
Optic nerve access
COMPLICATIONS
Extreme care is required with this surgery due to the paranasal sinus’ proximity to the orbits, brain, internal carotid arteries, and optic nerves. However, even with these possible serious risks, there are many benefits to be reaped by a patient with appropriate indications from a well-performed FESS. As the degree of difficulty increases with these surgeries, a surgeon with appropriate experience must be present to manage the procedure. This is especially true in approaches to neurosurgical procedures. You may classify to:
Orbital complication: including orbital haemorrhage, abscess, damage to optic nerve
Intracranial complication: including CSF Leak, meningitis, Brain abscess, Intracranial haemorrhage
Nasal complication: including adhesion formation, anosmia, hyposmia, injury to lacrimal duct.
PATIENT INFORMATION POST OPERATIVELY
It is imperative that the nose is not blown hard for at least 48 Hours. There might be a bloody/watery discharge from the nose, which can be gently wiped. Swelling should be minimal. In isolated cases one eye or both could be slightly bruised. There should be slight pain, but not dramatically so. A follow up visit must be made for seven days postoperatively.
Usually antibiotics are given, which must be taken diligently.
From the third day onwards, the nose can gently be douched with Normal Sterile Saline, which must be bought from the pharmacy
Grommets
Although Myringotomy with tube insertion can be performed under local anaesthesia during a regular doctor’s appointment in co-operative adults, patients requiring tube insertion are very often young children. Since damage to the ear is possible unless the patient stays quite still while being manipulated, for any patient who may have difficulty lying still during the procedure, Myringotomy and tube insertion is performed under a brief general anaesthetic.
The insertion of tympanostomy tubes is one of the most common surgical procedures performed on children. It is the most common reason for a child to undergo a general anaesthetic. When the tubes are released from the ear, it is usually covered in wax. Nausea and vomiting is very common when the tubes fall out (as a result of equ8ilibrium that may need to pressurize the balance of the ear). It may last for up to 48 hours on some occasions.
Tympanostomy tubes generally remain in the eardrum for some period of time, ranging from 2 months to a year, before spontaneously falling out of the eardrum. The eardrum usually (but not always) closes without a residual hole at the tube site.
POST-OPERATIVE
A blood stained or watery discharge from the ear for the first couple of days is a normal occurrence.
Use medication as prescribed.
Make an appointment for a post-operative follow up examination 10-14 days after the operation
Avoid getting any water in the ears. Cotton wool with Vaseline plugs or “prestick” or any other effective plug must be used, when swimming or exposure to water. A Flipper band with silicone plugs is available at my consultation rooms or at the Hearing and Balance Clinic, House 13, Garden City Clinic.
Meatoplasty
This causes water and wax to accumulate on the inside and not to be able to extrude, followed by recurrent ear infections.
TECHNIQUE (SURGICAL)
A Meatoplasty procedure is done under anaesthetics.
The skin of the ear canal is lifted up and the bony portion is drilled open, whereafter the skin is replaced. It has a high rate of success and with the right indications, gives great relief to people with chronic infections.
Myringoplasty
There are several options for treating a perforated eardrum. If the perforation is from recent trauma, many ear, nose and throat specialists will elect to watch and see if it heals on its own. After that, surgery may be considered.
Dr Rossouw has a myringoplasty/Tympanoplasty technique for small central perforations which can be done through the canal with no incision, and a small graft of cartlidge taken from the inside of the ear, is used to plug the hole. This procedure can be performed in younger patients with perforations and chronic middle ear infections as it is very non-invasive. The patients are mostly discharged the same day and the success rate is very high. More than a hundred of these operations have been performed by the surgeon. Dr. Rossouw spend time working with Joachim Hearman, well known German Surgeon in Germany, who pioneered cartlidge used in closing of eardrum perforations.
When the normal anatomy of the middle ear has been destroyed by either infection or cholesteatoma, the connection of the eardrum with the inner ear has to be re-established. Various prosthesis are used in this instance depending on the problem. Sometimes the patient’s own tissue or ossicles are remodelled and used. If a reconnection can be established and maintained, the results are generally extremely satisfying. Often if an infection is present, this is first managed and at a second stage the hearing can be attended to and an attempt to repair that, can be considered.
Mastoidectomy
SURGICAL APPROACH
Tympanoplasty / Mastoidectomy can be performed through the ear canal (trans canal approach), through an incision in the ear (end aural approach) or through an incision behind the ear (post auricular approach).
A graft may be taken to reconstruct the tympanic membrane. Common graft sites include the temporalis fascia and the tragus.
The surgery takes ½ to 1 hour if done through the ear canal and 2½ to 3 hours if an incision is needed.
For any further information, please contact the practice of Dr. Deon Rossouw at dprossouw@samedical.co.za.
Nasal Fracture Reduction
The prototypical patient is a male aged 15 – 30 year who was involved in a fight, motor vehicle accident or fall.
Approximately 80% of nasal fractures occur between the thicker proximal and thinner distal segment of the nasal bones. Although frontal impact can cause fracture of the nasal bones, lateral impacts are more common. These lateral impact injuries typically cause a depression of one nasal bone and may result in a lateral displacement of the contralateral nasal bone.
DIAGNOSIS
The diagnosis is mostly made by clinical examination and the history. Sometimes x-rays or a C.T-Scan is done to confirm the diagnosis.
In severe facial injuries x-rays are done to confirm other injuries or fractures of the face as well.
Usually nasal fractures are accompanied by a bleeding of the nose due to a tear of the mucus membrane on the inside of the nose.
TREATMENT
Minor nasal fractures need only to be treated with pain medication and anti-inflammatory. Antibiotics are usually given as the mucus membrane on the inside is often torn, exposing the fracture to the inside of the nose and thus a higher risk of infection.
Mild fractures without much displacement can usually be manipulated by a professional min the field, under local anaesthetic, in an out-patient or surgery environment.
More serious nasal fractures are usually accompanied with deviations of the septum that combine reduction of the nasal fracture as well as a septal reduction is done under anaesthetics.
Severely fractured nose usually need to have a cosmetic Septo-Rhinoplasty done at a later stage, if the initial manipulation does not achieve a satisfactory cosmetic or functional result.
Rhinoplasty
Often a nasal hump can be removed or a tip of the nose can be structured to have a more pleasing look.
Most medical aids pay for Rhinoplasty procedures if they are purely functional in nature. If they are cosmetic, a co-payment from the patient is usually necessary. This can be discussed with the accounts department.
A host of other patients that have been done, with pre-operative and post-operative pictures are available for perusal should a patient consider having a Rhinoplasty done in this practice.
Septumplasty
Because a deviated nasal septum often compromises the airflow through the nose it can induce snoring. This is often the first step in controlling of snoring apart from the other entities like losing weight, etc.
PROCEDURE
The procedure usually involves a judicious excision/realignment of a portion of the bone and/or cartilage in the nasal cavity. Under general or local anaesthesia, the surgeon works through the nostrils, making an incision in the lining of the septum to reach the cartilage targeted in the operation. Sufficient cartilage is preserved for structural support. After the septum is straightened, it may then be stabilized temporarily with small plastic tubes, splints, or sutures internally.
POST-OPERATIVE
Unless there are unusual complications, there is no swelling or discoloration to the external nose or face with Septoplasty alone. Often the nose needs to be packed with a small sponge for a couple of hours postoperatively to ensure that bleeding is kept under control. However under certain circumstances this is not necessary. One percent of patients can experience excessive bleeding afterwards- the risk period lasts up to two weeks. This could require packing or cautery, but is generally handled safer and without compromise of the ultimate surgical result.
Stapedectomy
Significant contributions to modern Stapedectomy techniques were then made by the late Dr. Antonio De La Cruz of the House Ear Institute in Los Angeles (Dr Rossouw spent time with Dr De La Cruz in Los Angeles in 1988); by the late Professor Henry Andre Martin of the Hospital Edouard Herriot in Lyon, France, including calibrated platinotomy (stapes footplate rather than whole surgery) and trans-footplate piston surgery that also paved the way for modern stapedotomy; and by the late Dr. Jean-Rene Causse of the eponymous clinic in Beziers, France, who pioneered the use of Teflon piston prostheses (also critical progress for stapedotomy) and, with his late son Dr. Jean-Bernard Causse, the reattachment of the stapedius muscle alongside the use of veinous grafts (Dr Rossouw has visited the Causse Clinic in Beziers on three previous occasions). In recent decades, Dr. William H. Lippy of the Lippy Group for Ear, Nose and Throat in Warren, Ohio has also claimed multiple advances of the surgical procedure.
If the stapes footplate is fixed in position, rather than being normally mobile, then a conductive hearing loss results. There are two major causes of stapes fixation. The first is a disease process of abnormal mineralization of the temporal bone called otosclerosis. The second is a congenital malformation of the stapes.
In both of these situations, it is possible to improve hearing by removing the stapes bone and replacing it with a micro prosthesis – a Stapedectomy, or creating a small hole in the fixed stapes footplate and inserting a tiny, piston-like prosthesis – a stapedotomy. The results of this surgery are generally most reliable in patients whose stapes has lost mobility because of otosclerosis. Nine out of ten patients who undergo the procedure will come out with significantly improved hearing while less than 1% will experience worsened hearing ability or deafness. Successful surgery usually provides an increase in hearing ability of about 20dB. That is as much difference as having your hands over both ears, nor not. However, most of the published results of success fall within the speech frequency of 500 Hz, 1000 Hz and 2000 Hz; poorer results are typically obtained in the high frequencies, but these are normally less hampered by otosclerosis in the first place.
INDICATIONS
Indications of Stapedectomy;
Conductive hearing loss (due to fixation of stapes)
Air bone gap of at least 30 dB.
Presence of Carhart’s notch in the audiogram of a patient with conductive hearing loss (relative)
Good cochlear reserve as assessed by the presence of good speech discrimination.
CONTRAINDICATIONS
Contraindications for Stapedectomy;
Poor general condition of the patient.
Only hearing ear.
Poor cochlear reserve as shown by poor speech discrimination scores.
Patient with tinnitus and vertigo.
COMPLICATIONS
Complications of Stapedectomy;
Facial palsy
Vertigo in the immediate post of period
Vomiting
Perilymph gush
Floating foot plate
Tympanic membrane tear
Dead labyrinth
Perilymph fistula
Labyrinthitis
Granuloma (Reparative)
Tinnitus
When a Stapedectomy is done in a middle ear with a congenitally fixed footplate, the results may be excellent but the risk of hearing damage is greater than when the stapes bone is removed and replaced (for otosclerosis). This is primarily due to the risk of additional anomalies being present in the congenitally abnormal ear. If high pressure within the fluid compartment that lies just below the stapes footplate exists, then a perilymphatic gusher may occur when the stapes is removed.
Stapedotomy
Laser stapedotomy is a well-established surgical technique for treating conductive hearing loss due to otosclerosis. The procedure creates a tiny opening in the stapes (the smallest bone in the human body) in which to secure a prosthetic. The CO² laser allows the surgeon to create very small, precisely placed holes without increasing the temperature of the inner ear fluid by more than one degree, making this an extremely safe surgical solution. The hole diameter can be predetermined according to the prosthesis diameter. Treatment can be completed in a single operation visit using anaesthetics, normally followed by one or two night’s hospitalization with subsequent at-home recovery time a matter of days or weeks.
Tonsillectomy
INDICATIONS
Tonsillectomy may be indicted when the patient:
Experiences recurrent infections of acute tonsillitis. The number requiring tonsillectomy varies with the severity of the episodes. One case, even severe, is generally not enough for most surgeons to decide tonsillectomy is necessary. Paradise in 1983 defined recurrent tonsillitis warranting surgery by the attack frequency standard as “three or more attacks of sore throat per year despite adequate medical therapy”.
Has chronic tonsillitis, consisting of persistent, moderate-to-severe throat pain.
Has multiple bouts of peritonsillar abscess.
Has sleep apnea (stopping or obstructing breathing at night due to enlarged tonsils or adenoids)
Had difficulty eating or swallowing due to enlarged tonsils (very unusual reason for tonsillectomy)
Produces tonsillo liths (tonsil stones) n the back of their mouth.
Have abnormally large tonsils with crypts (Craters or impacts in the tonsils).
CONTROVERSY OVER INDICATIONS
The American Academy of Otolaryngology & Head and Neck Surgery (AAO-HNS) stated that “In many cases, tonsillectomy may be a more effective treatment, and less costly, than prolonged or repeated treatments for an infected throat…. For the past several years, the Academy has been developing clinical guidelines based on evidence and outcomes research, including ‘Quality of Life after Tonsillectomy, ’a January 2008 supplement to the journal Otolaryngology-Head and Neck Surgery.”
MORBIDITY AND MORTALITY
The morbidity rate associated with tonsillectomy is 2 to 4% due to post-operative bleeding; the mortality rate is 1 in 15,000, due to bleeding, airway obstruction, or anaesthesia.
POST-OPERATIVE CARE
Although the throat is very painful post-operatively, it is imperative that the patient should eat and drink fluids for the first 24 Hours. A soft diet is recommended i.e. jelly and ice cream etc. thereafter, the patient must gradually return to a normal diet, keeping in mind that strong spices i.e. curries and fruit, especially bananas may aggravate the discomfort.
A sore throat will persist for around two weeks after the operation. Most patients do not feel like swallowing anything during the first few days after surgery. Patients should try to get as much cold fluid down as possible, as it will help speed recovery. Very cold drinks will help bring down swelling. Ice cream, frozen yogurt puddings, slushies, sorbet and popsicles, on the other hand, are recommended. Large quantities of ice should be prepared in advance.
Pain following the procedure is significant and may include a hospital stay. Recovery can take from 10 up to 20 days, during which potent analgesics are typically prescribed. Patients are encouraged to maintain diet of liquid and very soft floods for several days following surgery. Rough textured, acidic or spicy foods may be irritating and should be avoided. Proper hydration is very important during this time, since dehydration can increase throat pain, leading to a vicious circle of poor fluid intake.
At some point, most commonly 7-11 days after the surgery (but occasionally as long as two weeks (14days) after), bleeding can occur when scabs begin sloughing off from the surgical sites. The overall risk of bleeding is approximately 1%-2% higher in adults. Approximately 3% of adult patients develop significant bleeding at this time. The bleeding might naturally stop quickly or else mild intervention (e.g., gargling cold water) could be needed (but ask the doctor before gargling because it might bruise the area of the skin that has been cauterized). Otherwise, a surgeon must repair the bleeding immediately by cauterization, which presents all the risks associated with emergency surgery (primarily the administration of anaesthesia particularly on a patient whose stomach may not be empty).
Generally speaking, tonsils will be removed if a patient needs antibiotics to be prescribed three times a year for tonsillitis, and the general practitioner’s recommendation is based on how the quality of life will be improved after the operation. Tonsillectomies can be performed while the patient is actually suffering from tonsillitis; however this increases the risk of bleeding.
COMMON CAUSES, DEMOGRAPHICS
Infections requiring tonsillectomy are often a result of Streptococcus (“strep throat”), particularly Streptococcus pyogenes; some may be due to other bacteria, such as Streptococcus viridans, St0phylococcus aureus, and Haemophilus influenza. However, the etiology of the condition is largely irrelevant in determining whether tonsillectomy is required.
Most tonsillectomies are performed on children, although many are also performed on teenagers and adults, it is the most common major surgical procedure performed on children. The number of tonsillectomies has dropped significantly from over a million cases per year in the 1950’s to approximately 600 000 in the late 1990’s. This has been due in part to more stringent guidelines for tonsillectomy and adenoidectomy (see tonsillitis and adenoid). Still, debate about the usefulness of tonsillectomies continues. Enlarged tonsils are removedmore often among adults and children for sleep apnea (airway obstruction while sleeping), snoring, and upper airway obstruction. Children who have sleep apnea can do poorly in school, are tired during the day, may be bedwetters beyond what is normal, and have some links to ADHD.
Tonsillectomy in adults is more painful than in children, although each patient will have a different experience. Various procedures are available to remove tonsils, each with different advantages and disadvantages. Children and teenagers sometimes exhibit a noticeable change in voice after the operation.
SURGICAL PROCEDURE
The generally accepted procedure for tonsillectomy involves separating and removing the tonsils from the subcapsular plane – a fascia of tissue that surrounds the tonsils. Removal is typically achieved using a scalpel and blunt dissection or with electrocautery, although harmonic scalpels or lasers have also been used. Bleeding is stopped with electrocautery, ligation of sutures, and the topical use of thrombin, a protein that induces blood clotting.
The procedure is carried out with the patient lying flat on their backs, with the shoulders elevated on a small pillow so that the neck is hyperextended – the so-called ‘Rose’ position. A mouth gag is used to prop the mouth open; if an adenoidectomy is also being performed, the adenoids are first removed with a curette; the nasopharynx is then packed with sterile gauze. A tonsils is removed by holding it by the upper part, pulling it slightly medially, and making a cut over the anterior faucial pillar. After the tonsil is removed from its position, a snare can be used to make a small cut on the lower portion prior to removal of the tonsil. The use of electrocautery minimizes the blood loss.
OTHER METHODS
The scalpel is the preferred surgical instrument of many ear, nose and throat specialists. However, there are other procedures available – the choice may be dictated by the extent of the procedure (complete tonsil removal versus partial tonsillectomy) and other considerations such as pain and post-operative bleeding.
HISTORY
The tonsillectomy has been practiced for 3,000 years, with varying popularity over the centuries. The procedure is first mentioned in “Hindu medicine “about 1000 BC; roughly a millennium later the Roman aristocrat Aulus Cornelius Celsus (25 AD-50 AD) described a procedure whereby using the finger (or a blunt hook if necessary), the tonsil was separated from the neighbouring tissue prior to being cut out. Galen (121 – 200 AD) was the first to advocate the use of the surgical instrument know as the snare, a practice that was to become common until Aetius (490 AD) recommended partial removal of the tonsil, writing “Those who extirpate the entire tonsil remove, at the same time, structures that are perfectly healthy, and, in this way, give rise to serious Haemorrhage”. In the 7th century Paulus Aegineta (625 – 690) described a detailed procedure for tonsillectomy, including dealing with the inevitable post-operative bleeding. 1,200 years pass before the procedure is described again with such precision and detail.
The middle Ages saw tonsillectomy fall into disfavour; Ambroise Pare (1509) wrote it to be “a bad operation “and suggested a procedure that involved gradual strangulation with a ligature. This method was not popular with the patients, however, due to the immense pain it caused, and the infection that usually followed. Scottish physician Peter Lowe in 1600 summarized the three methods in use at the time, including the snare, the ligature, and the excision. At the time, the function of the tonsils was thought to be to absorb secretions from the nose; it was assumed that removal of large amounts of tonsillar tissue would interfere with the ability to remove these secretions, causing them to accumulate in the larynx, resulting in hoarseness. For this reason, physicians like Dionis (1672) and Lorenz Heister censured the procedure.
In 1828, physician Philip Syng Physick modified an existing instrument originally designed by Benjamin Bell for removing the uvula; the instrument, known as the tonsil guillotine (and later a tonsillotome), became the standard instrument for tonsil removal for over 80 years. By 1897, it became more common to perform complete rather than partial removal of the tonsil after American physician Ballenger noted that partial removal failed to completely alleviate symptoms in a majority of cases. His results using a technique involving removal of the tonsil with a scalpel and forceps were much better than partial removal; tonsillectomy using the guillotine eventually fell out of favour.
IMMEDIATE POST-OPERATIVE CARE
Under no circumstances must any form of aspirin be taken (or any other anti-inflammatory medication, in effect Brufen, Myprodol, Voltaren, Nurofen, Grandpa, etc), as this can precipitate bleeding from the tonsil bed (due to an effect on the blood coagulation. Most postoperative bleeding is caused by ingestion of the above and dehydration, secondary to the patient not taking in enough fluid. A rough ballpark figure on the amount of fluid that the patient should be taking is approximately 50ml per kilogram of body mass per 24 Hours in children under the age of 10. Over the age of 10, 1.5 litres a day is usually the norm.)
If at any stage post-operatively the patient bleeds fresh blood from the mouth, or nose, (take the patient to Garden City Clinic’s Casualty Department, where they will stabilise the patient and contact Dr. Rossouw, or contact Dr. Rossouw on his emergency number on 072 9883 136 code 00001)
Tympanoplasty / Mastoidectomy
CLASSIFICATION
Tympanoplasty is classified into five different types, originally described by Wullstein in 1956.
Type 1 involves repair of the tympanic membrane alone, when the middle ear is normal. A type 1 Tympanoplasty is synonymous to myringoplasty.
Type 2 involves repair of the tympanic membrane and middle ear in spite of slight defects in the middle ear ossicles.
Type 3 involves removal of ossicles and epitypmanum where there are large defects of the malleus and incus. The tympanic membrane is repaired and directly connected to the head of the stapes.
Type 4 describes a repair when the stapes foot plate is movable, but the crura are missing. The resulting middle ear will only consist of the Eustachian tube and hypotympanum.
Type 5 is a repair involving a fixed stapes footplate.
Your Health Starts Here
call — +27 (0) 11 839 4418 / 9